Hapless Bills Fan
-
Posts
48,720 -
Joined
-
Last visited
Content Type
Gallery
Profiles
Forums
Events
Everything posted by Hapless Bills Fan
-

Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
I mean, you can say that, but WTF man? these aren't numbers the CDC pulled out of their keister. They're two separate studies of thousands of people, with the data collected and reviewed by all the authors, and then available upon request. They all signed their work. Then you have to look at the NFL's preseason numbers and public health UK with two peer-reviewed published studies, and all those are consistent. So you can believe what you like, but there really ought to be a higher standard of rebuttal than "I don't believe it, those data are ***** up". There's a preprint up that has gotten a lot of press and that I have questions and am skeptical about, and my reasons are because they pulled an 18,000 person sample out of 2.5 million people and whenever someone does that to avoid bias, it's legitimate to question whether the sample introduced bias in some other way and to wonder what the raw 2.5 million dataset would look like; I don't just say "I don't believe the other stats, not for a freakin' second". -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
The key question is “when?” I believe that was true in Spring and may still be true in some places where vax levels are high like MD MA NY It’s so far from true in rural MO and GA this summer that it’s laughable. Boots on the floor accounts. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
This is great info and thanks for the details, I’m gonna do it today -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
NFL data 7x less likely to be infected. No intra-facility spread. CDC LA study. 5x less likely to be infected, 29x less likely to be hospitalized. CDC HCW study ( high exposure) when tested weekly, all infections 3x less likely with some evidence of declining effectiveness after 6 months. UK public health 5x less likely. These all with Delta. The vaccine reduces spread -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
I don't think it's an unreasonable concern to bring up, but at this point it's been brought up and addressed and brought up and addressed. Which to me moves it from a concern, to an excuse. But maybe you're right and I'm wrong and there isn't actually a lot out there that does a good job of debunking this, especially if you were looking at a reasonable site and got that impression. So I'm on it. I will put up front, though, that concerns which were reasonable a year ago IMO are a lot less reasonable a year later, with more than 200 million doses served in the US alone and full FDA approval. The big place the timeline got compressed was in development, and the reason it got compressed was by the nature of these two vaccines. They've been pursued for decades because they can be so fast. The manufacturing process is in place, the characterization tests are in place, you just stick in the DNA or mRNA for the protein you want to make as soon as the sequence is known (and it was known mid-January) and start testing in animals. The reason more traditional conjugated protein vaccines and inactivated virus vaccines took longer is that a unique manufacturing process and to some extent unique characterization tests have to be developed and vetted for each new vaccine. In this case, the development further accelerated because they used learnings from vaccine development for the similar SARS and MERS. They took a protein mutation that locks the spike protein in the pre-bound state, the idea being it would develop better neutralizing antibodies (antibodies that prevent binding to cells) that way. That wasn't the only thing they tried of course - I think the initial animal studies were at least 50 different candidates and Pfizer actually took 4 different candidates through early clinical trials. But it's not uncommon for scientists to spend several years testing different proteins or pieces of protein to see what will give them the desirable immune response and avoid undesirable responses, in animal models. Here they used prior knowledge to go right for the gold. The combining of clinical trials is actually NBD for a vaccine, and the reason it isn't done more often is really risk to the company, not safety. With drugs, phase I is safety and phase II is "first in patient", the readout on whether the drug actually works and large-scale development should continue. With vaccines, because the point is to give them to healthy people and get an immune response, you look for immune response and get initial "does it work?" info from Phase I. But still, most companies want to make just enough material for Phase II and get a larger readout before they go "full speed ahead". Phase II material is usually made at a small pilot plant under the same strict regulations as clinical manufacture. The FDA requires that phase III trials must use the exact manufacturing process you intend to use for commercial manufacture and take place at the same facilities. Any improvements in yield or purity or length, do it before Phase III. So normally you complete Phase II and get an initial readout on how the drug or vaccine works, THEN start scaling up the manufacture. In this case, the manufacturers said "damn the cost, we're gonna go right from Phase I to clinical manufacture. Moderna said it because they took money from President Trump's Operation Warpspeed and Dolly Parton etc etc. so it wasn't entirely their dime if it fizzled. Pfizer did it because Bourla (CEO) told them to and because they have the deep pockets (didn't take external development money). It was a huge financial risk But from a safety viewpoint it was no big deal because you don't enroll and inject 40,000 people all at once, you enroll and inject about the same number of people you would in a normal phase II trial and just put in a benchmark where you package up the data you collect on that subset and go over it with a fine tooth comb looking for safety concerns as well as efficacy, then give it to the FDA to comb while meanwhile you continue enrolling volunteers and inject as soon as you get the green light to proceed. But the pause to finalize and scale up manufacture and produce commercial-grade vaccine wasn't there, because they used the manufacturing process and commercial grade production for phase II. I was actually part of the Phase III clinical trial for Rubella vaccine in 1968. Rubella is 100% non-fatal disease which half the infected people didn't know they had, and the only way the vaccine was going to do what it was intended to do (prevent infection during early pregnancy) was if vaccination were widespread. We all lined up and got vaccinated, "save the babies". But back in the 1960s when people were actually seeing the ravages of many of the diseases for which vaccines are common in the wild, there was general agreement that vaccines were a Public Benefit. Someone who suggested they were gonna wait an extra 6 years to get injected because that's how long development ought to take and it was suspicious - what corners did they cut to develop the vaccine so fast? would probably have been regarded as a bit anti-social. We were proud of science and technology and welcomed scientific advances, and we were community-minded. As for "why now", development took place for SARS and for MERS and for Ebola, but none of those diseases took off and became a global threat. They weren't that contagious. There's been development for cancer treatments, and development for flu, but with flu they're going up against an established vaccine with an established safety record, so the bar is higher, and the acceptance is lower. Hope this helps, and fair warning, I may split this off to the Off the Wall thread.- 846 replies
-
- 10
-

-

-

-
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Good question. Looking at the schedule: lotta vaccinated folks around Washington/MD, WFT fans could buy. Ditto NE, could be sales to Chowdaheads. Jets fans? Do Jets fans want to travel to support their team? If it's exciting and good perhaps. With Dolphins, Texans, Colts, and Panthers fans - travel to a vaccine-requiring stadium may not be a selling point. I'm not sure about Atlanta fans. Where do they draw from? -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Good point. But being a bit Devil's Advocate here, if everyone going into the stadium is either vaccinated or tests negative, the odds of being infected inside the stadium are probably pretty low. There seem to have been some outdoor mass events (Lollapalooza) where vaccination/negative test were the standard and epidemiologists concluded there was no evidence of mass spread. I suspect that the logistics of testing that many people would be formidable. It appears to me from the NY Forward dashboard that the largest number of tests WNY has been performing in 1 day was ~15,000 and that was an outlier, it's usually more like 3,000-5,000. 40% of 70,000 would be 28,000 tests. So that may be a "fail" on logistics and supply reasons, but if it could be pulled off it would certainly be less controversial. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
See, this sort of thing just bugs the snot out of me to read, no offense. Back in Da Da when a lot of the vaccines were developed - polio, measles, mumps, rubella - the tools and tests available to vaccine developers were laborious and slow. We have had several revolutions in biological and biopharma techniques in my working lifetime. What used to take 2 years can sometimes be done in 2 weeks. It's sort of like saying "Historically, it took 200 years to build a cathedral, I don't trust buildings that were constructed in 2 years" Modern construction techniques make more rapid timelines possible, so why is a Medieval cathedral construction timeline relevant? The whole idea of adenovirus vector and mRNA vaccines was a template that an emerging disease can be "plugged in" to. Being able to do it fast was the point, to be able to fight a pandemic. Scientists have been working towards this for literally, decades. Now it's like they're being criticized for perceiving a need decades ago, making advances , and working their asses off to put the thing together in a month and start the full cohort of animal and human safety studies quickly. There's really nothing admirable about insisting you can only trust buildings constructed with a stone chisel and a treadwheel crane because anything built faster must be unsafe, by reason of being built faster. Anyway while I appreciate the civil tone going on, we're getting pretty general here, could we narrow it back to football relevance? I get it, some people feel they don't need to be vaccinated because their pristine and magnificent personal state of health makes them unlikely to suffer serious ills. Hopefully right, maybe wrong, but either way shirks the question of spreading illness to others. Natural immunity has been shown to be boosted by a vax, so there's that. But if you don't want the vax and it keeps you out of the stadium, absolutely your right. -
Week 2: Bills at Dolphins
Hapless Bills Fan replied to YoloinOhio's topic in The Stadium Wall Archives
You're too deep for me, I can see no connection between protecting 3 practice squad players and the above, unless you're trying to make a flaccid case that the Bills coaches and FO have a uniform incompetence. Which would be foolish, so I hope you're not doing that. Grrrrrrrrr -
Week 2: Bills at Dolphins
Hapless Bills Fan replied to YoloinOhio's topic in The Stadium Wall Archives
That's strange, why wouldn't we protect 4 if that's what's allowed? -
Alpha's Good, the bad, and the ugly week 1...
Hapless Bills Fan replied to Alphadawg7's topic in The Stadium Wall Archives
I agree, but I think there's also a point that sometimes there were short throws available and Allen passed them up in favor of the deeper plays. I think that's going to be an issue because the league has the memo that Allen hates to take the checkdown. So they smother the other guys and leave the checkdown or hot read enough green around them to plant a Christmas tree farm, and that's how it's going to be until Allen wraps his mind around the need to make them pay for it. OK, but the thing is, if the OL isn't getting 'er done, how about bringing in a TE and and RB (or 2 TE, or an extra OLman) to help block, instead of running 4 and 5 WR sets almost half the game (and leaving Singletary out wide a lot)? The play calling plays a role. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
I know it's a nit, but a) one of the vaccines is fully approved now 2) a vaccine is not a drug I also live in Missouri with relatives and friends in 3 of the least vaccinated counties in the State. I know a lot of people who say exactly what you say. Some of them caught covid and NBD, some got very sick. some when to hospital and it's "knew them" now for too many. My niece is an RN and works in the ICU of a small county hospital. She is unvaccinated, her choice. We're terrified for her because of all the deaths of people in her age group (30-40) and her high exposure. It would devastate her 5 children, her disabled husband, and her parents if anything happened to her. I'm not trying to argue you. Just be sure you choose on facts and not misinformation. The smartest people change their mind all the time in the face of new information. Godspeed. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Do you think the stadium workers are not being required to get the vaccine? I agree with you if true. If you mean the players, well, The Union Makes Us Strong. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Almost certainly Hepatitis B. Almost certainly the recombinant vaccine if you were vaccinated after 1986 - no human plasma involved in that one. Some colleges require or recommend Hepatitis A, and some pediatricians recommend it -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
@Buffalo716, I expect if there was a serious outbreak of these other diseases going on (TB, say) there would be testing for them for sure, or a push to vaccinate people if a vaccine exists. And the diseases you mentioned are a lot harder to transmit. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
You're both right. There are 5 different Hepatitis viruses A, B, C, D, and E. Hepatitis A and E are passed through contamination, usually fecal, of food or water. "A" is probably what your Cheektowaga worker had. Hepatitis B and C are passed through blood or body fluids. "D" coinfects along with B. There's a very effective vaccine to prevent Hepatitis A, and in a number of counties in MO, all food service workers are required to be immunized for Hep A in order to be employed in that field. I'm actually kind of surprised Erie County doesn't require it. There's a very effective vaccine to prevent Hepatitis B also, and most hospitals and employers require employees who work with blood or OPIM (other infectious materials) to be vaccinated. This is "risk management" because Hep B becomes a chronic infection leading to liver failure or liver cancer in about 6% of infected adults, which would kick insurance claims through the roof. Now there's a safe recombinant vaccine and it's routinely given to infants (90% of infected infants develop chronic infection). But when the first vaccine came out, it was a gut-check because the virus was isolated from the plasma of Hep B infected humans then purified and inactivated. Those Hep B infected humans were often co-infected with HIV. We had to really be persuaded to trust the science and trust the process. Some people quit. I took 5 injections to seroconvert. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
OK, so the US plan calls for an option Erie County decided not to take. Would love to be a fly on the wall and understand what discussions were behind that. I"m not going to assume not public health based. But it's interesting. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
I think it is natural to have reservations, and I think the CDC has done a poor job of communication. But there are mountains of misinformation and that is a problem. The "generally accepted risk groups" notion portrays vaccination as a "me only" choice rather than a societal benefit. And that's all I'll say here - not the place for a general debate. You wouldn't have been the 3rd or the 4th to make that quip here -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
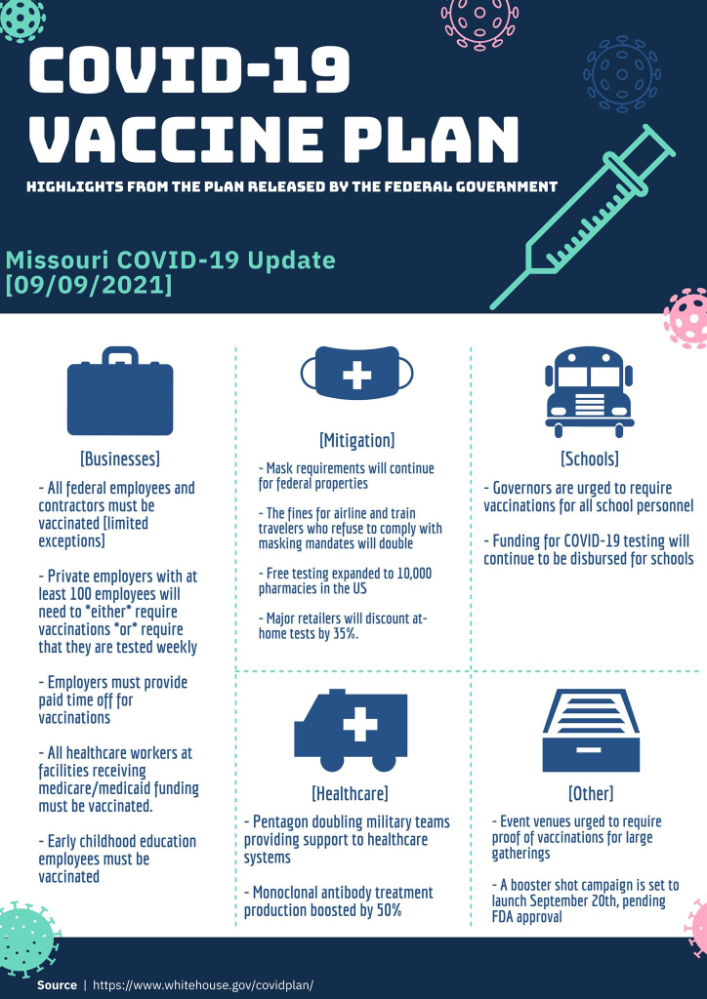
I don't think it's a rule, so I think the Bills/County do have a say. Here's a summary of the US plan from a source I consider trustworthy (click to embiggen): It just says that large event venues are URGED to require proof of vaccination, it doesn't say they're required to require them (that's ponderous, but you get me I hope) Someone pointed out that NY just enacted a ruling Sept 6 that Covid is an airborne disease for which businesses are required to provide a transmission prevention plan. I think it might be a reasonable guess that Erie County/Highmark Stadium quickly came up with a plan involving "mask indoors/unvaccinated mask". Well, Sept 12 was pretty strong proof that wasn't going to work. So, Next Plan....
-
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Couldn't find quickly, but looks pretty large capacity from this photo: https://www.atptour.com/en/news/us-open-2021-full-capacity -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Jack, clarification please: is this a list of apps that Highmark/Bills will accept or a just a general list? -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
I think you should look at the moon landing. Did we land on the moon, or no? -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
Truth. Peace out. -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
So how much of the stadium revenue is concessions, and how much is tickets? Anyone know? -
Highmark Stadium now requiring vaccination for entry
Hapless Bills Fan replied to StHustle's topic in The Stadium Wall
I think we're gonna be beating a dead horse here and will cause us to veer away from football PDQ if we keep this out. There are plenty of states with politically appointed public health 'experts' who don't think it's a problem and whose hospitals are jammed. I live in one of them. So I don't think that's a great argument for "it's not a problem" myself. You keep saying it's "obvious to you" but I don't think it's at all obvious overall. It's been shown at other venues that a combination of requiring vaccination and negative test results has worked OK for one-off events, but the same thing applies to your unvaccinated self - you could have tested negative while incubating an infection yesterday, or you could have had a false negative (especially with a rapid antigen test) so now we're back to "there's no telling whether that person (vaxxed or unvaxxed) has Covid or not" - so you go with the overall odds. We are NOT gonna go down the politics rabbit hole here, so just don't. You get a free pass on the "political leanings" and "Biden speech" stuff because you're responding to a post I made, but that's one.